
When thinking of gastric cancer, Helicobacter pylori (HP) is often the first culprit that comes to mind. However, in recent years, a growing body of research has revealed that the onset of gastric cancer may not originate solely within the stomach itself.
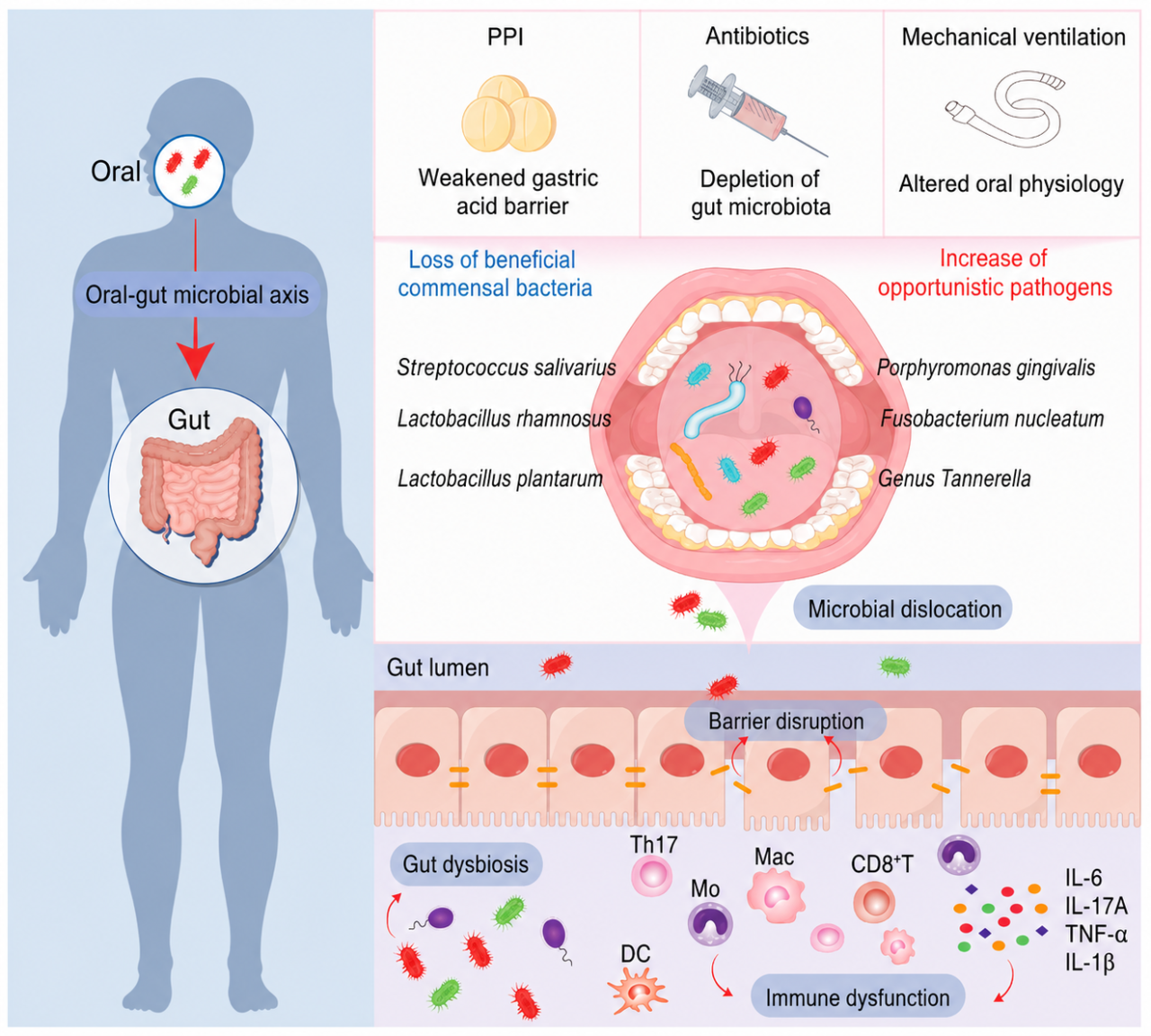
Bacteria in the oral cavity could be another overlooked driver: certain bacteria originally native to the mouth can "migrate" to the stomach, colonize in gastric cancer-associated environments, and drive carcinogenic progression through microbial synergy and metabolic alterations.
This bacterial pathway along the "oral-gastrointestinal axis" has once again sounded a new alarm for infection prevention and control in endoscopic examinations.
01 The "Invisible Drivers" of Gastric Cancer Progression
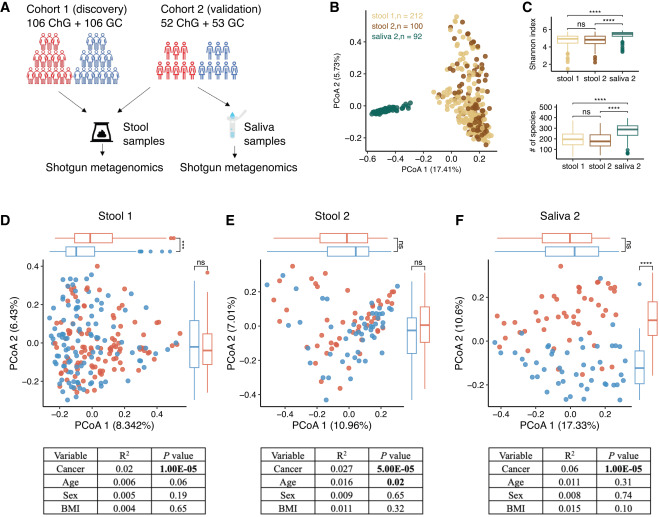
Recently, a research team led by Fang Jingyuan, an Academician of the Chinese Academy of Sciences from Renji Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, published a study in *Cell Reports Medicine*. The team performed metagenomic sequencing on 404 samples from 317 subjects, including saliva and fecal samples.
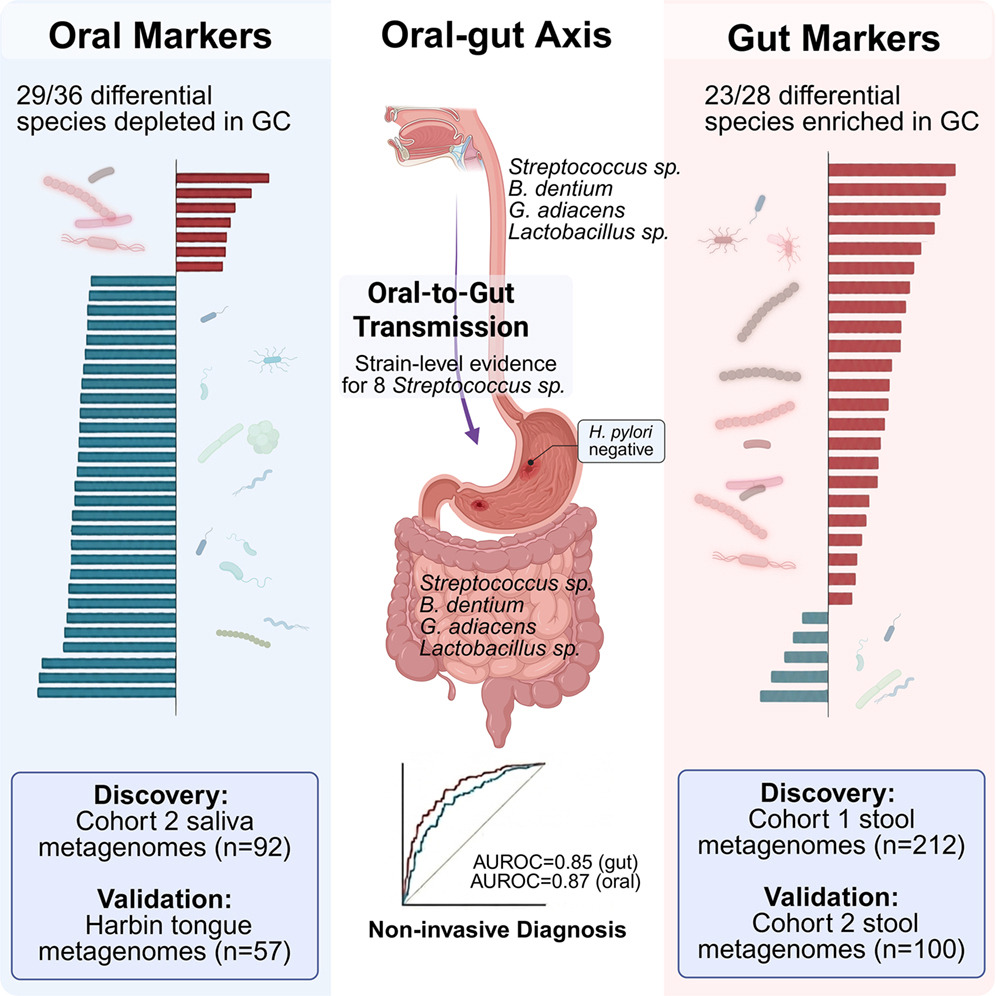
The research team discovered that among the 23 bacterial species enriched in gastric cancer patients, 20 were typical oral-colonizing bacteria.More crucially, 87 paired samples revealed that among 8 species of *Streptococcus*, the genetic similarity between strains derived from the same individual's oral cavity and gut exceeded 99.9%, confirming that these bacteria indeed migrate from the mouth to the intestinal tract.
Core Findings
- Key Strains:The genus *Streptococcus* is most closely associated with gastric cancer, with Streptococcus anginosus*being significantly enriched in the microbiota associated with gastric cancer patients.
- Carcinogenic Mechanism:** These bacteria form a synergistic microbial network that promotes lactic acid fermentation and acidifies the tumor microenvironment, thereby increasing gastric epithelial cell proliferation and malignant transformation.
This study has prompted the medical community to refocus on the potential impacts of "exogenous microbial migration" and "cross-site transmission."
In the field of digestive endoscopy, this implies that beyond traditional disinfection standards, how to further mitigate the risks of potential microbial transmission and reduce exogenous microbiota interference is becoming a new focus in infection control.
02 Endoscopic Infection Control Challenges Under the Risk of "Exogenous Microbiota"
The study unveils a "natural migration" pathway of bacteria from the oral cavity to the stomach. However, in clinical settings, endoscopic examinations artificially open up this very channel.
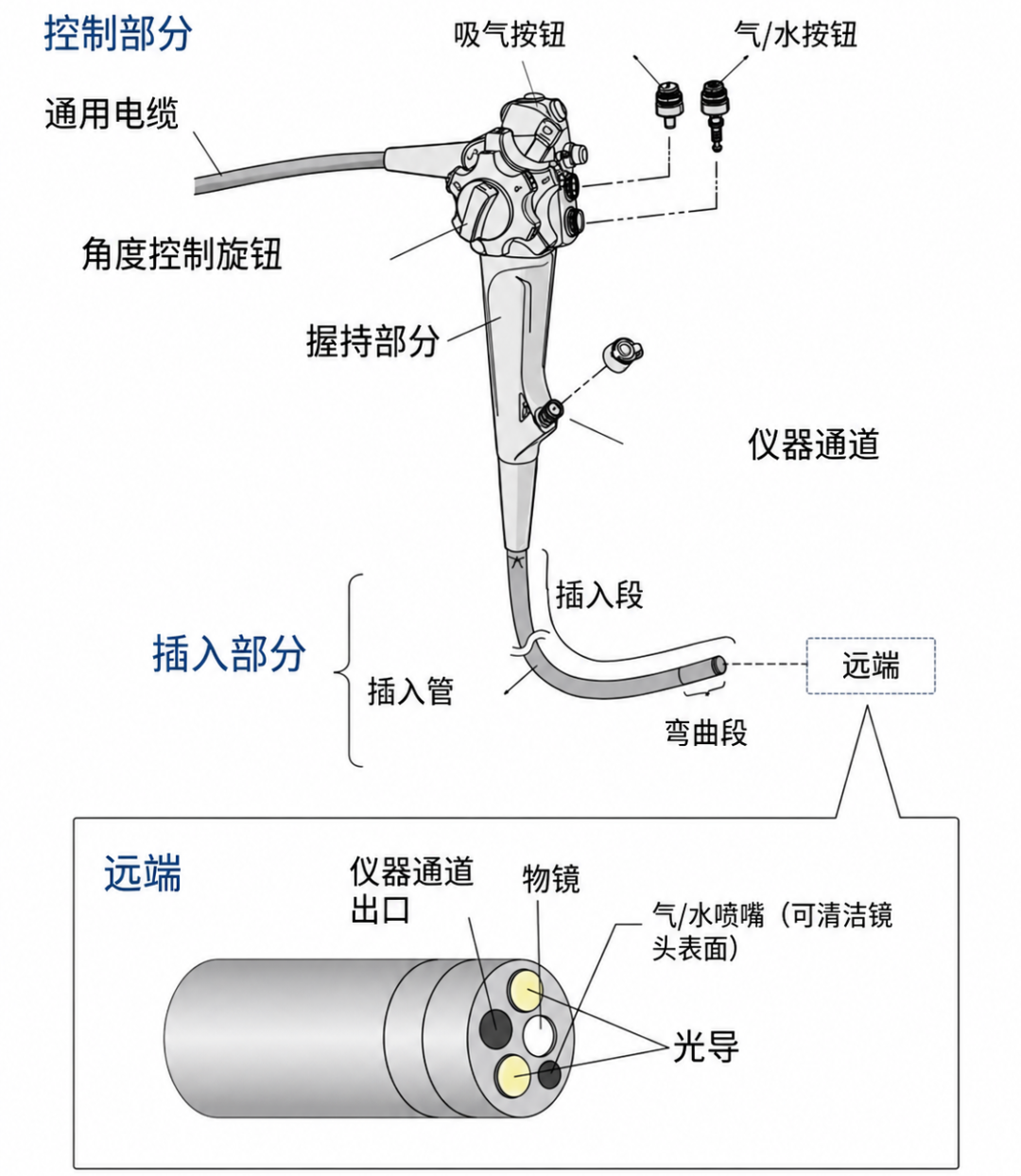
Role as a Vector: Although traditional endoscopes undergo standardized reprocessing after use, they inherently come into high-frequency contact with human mucous membranes and feature complex internal architectures. Their intricate components—such as lumens, nozzles, and bending sections—have always been primary targets of stringent management within global infection control frameworks across cleaning, disinfection, and drying procedures.
Despite the maturity of high-level disinfection (HLD) systems for endoscopes, risks of exposure to cross-contamination persist during transportation and storage. This model fundamentally relies on procedural compliance rather than the physical isolation of the device itself.With research now confirming the carcinogenic mechanisms of certain oral bacteria, the weight assigned to "infection risk" has been completely redefined.
This is no longer a matter of ordinary cross-infection; it potentially involves the cross-patient transfer of carcinogenic strains. Consequently, single-use endoscopes, characterized by a "one scope per patient, ready-to-use upon unpacking" model, are gaining renewed appreciation across an increasing number of clinical scenarios.
03 Clinical Value of EndoFresh® Single-Use Endoscopes
When traditional reprocessing encounters its operational boundaries, is there alternative path for infection control?
The core logic of single-use endoscopes lies in eliminating cyclical reprocessing and preventing the carrying of microbial residues from previous patients, thereby cutting off the possibility of endoscope-mediated transmission of exogenous bacteria at the source.
Isolation at the Source, Higher-Tier Infection Control: Each single-use endoscope is dedicated to a single procedure, entirely eliminating the issue of reprocessing residues.
Severing the Pathway of Carcinogenic Strains:Even if a patient harbors potential carcinogenic strains in the oral cavity, the endoscope will not serve as a vector for cross-patient bacterial transfer.
Adapting to More Complex Clinical Scenarios:Especially in settings such as ICUs, emergency rooms, high-infection-risk patients, perioperative care, multidisciplinary joint consultations, and mobile healthcare, single-use endoscopes are demonstrating increasingly robust clinical adaptability and workflow advantages.

As an innovative domestic single-use endoscope brand cleared by the US FDA, CE mark, and China NMPA, EndoFresh® products have reached numerous mainstream markets, including China, the United States, Europe, the Middle East, Southeast Asia, and Australia. Its solutions have achieved widespread recognition and clinical validation in routine examinations, complex surgeries, and diverse clinical applications.
Reflections
Infection control is not merely an upgrade of disinfection technologies; it is a fundamental restructuring of the underlying logic behind device selection.
As research unveils the deep connection between oral bacteria and gastric cancer, single-use endoscopes present an answer that commands serious attention: given that bacteria can migrate from the oral cavity to the stomach, traditional endoscopes might inadvertantly act as "transporters" of exogenous pathogens. In contrast, "one scope per patient, disposable" single-use endoscopes offer a safer new alternative for clinical infection control.
References
1. Zhang Y, et al. Oral-derived Streptococcus enrichment in the upper digestive tract promotes gastric carcinogenesis. Cell Reports Medicine. 2024.
2. Wang JY, et al. Streptococcus anginosus promotes gastric carcinogenesis through methionine metabolism. Gut. 2024.
3. World Health Organization (WHO). Decontamination and Reprocessing of Medical Devices for Health-care Facilities.
4. SGNA. Standards of Infection Prevention in Reprocessing of Flexible Gastrointestinal Endoscopes. Society of Gastroenterology Nurses and Associates.
5. ESGE & ESGENA Guideline. Reprocessing of flexible endoscopes and endoscopic accessories used in gastrointestinal endoscopy.
6. Bi YW, et al. A randomized controlled trial of single-use endoscopes in POEM treatment [J]. Chinese Journal of Digestive Endoscopy.
7. Fang Jingyuan’s Team: Interpretation of research findings on "Oral-derived Streptococcus enrichment and the mechanism of gastric carcinogenesis."